Table of Contents >> Show >> Hide
- The strange case that led to a scientific first
- What kind of tapeworm was found?
- Why sequencing the tapeworm genome mattered
- What the DNA revealed about treatment
- Sparganosis vs. neurocysticercosis: what readers should know
- How doctors diagnose brain parasite infections
- Symptoms that should never be ignored
- Prevention: boring habits that actually work
- Why this case changed parasite research
- The human side of the headline
- Experiences and practical reflections related to the brain tapeworm genome story
- Conclusion
A tapeworm in the brain sounds like the opening scene of a medical thrillerpossibly one with ominous violin music and a very nervous radiologist. But this real case did more than make readers squirm. It gave scientists a rare chance to study a mysterious parasite at the deepest biological level: its genome.
In a world first, researchers sequenced the genome of Spirometra erinaceieuropaei, a rare tapeworm removed from the brain of a man in the United Kingdom. The parasite had caused a condition known as sparganosis and had apparently migrated through the patient’s brain over several years before surgeons removed it. The discovery was medically fascinating, scientifically valuable, andlet’s be honestdeeply unsettling in the way only parasites can be.
Yet the story is not simply “man has worm in brain.” The bigger headline is what the worm’s DNA revealed. Sequencing its genome helped scientists identify the species, understand why diagnosis was so difficult, and look for clues about which anti-parasitic drugs might work against similar infections in the future.
The strange case that led to a scientific first
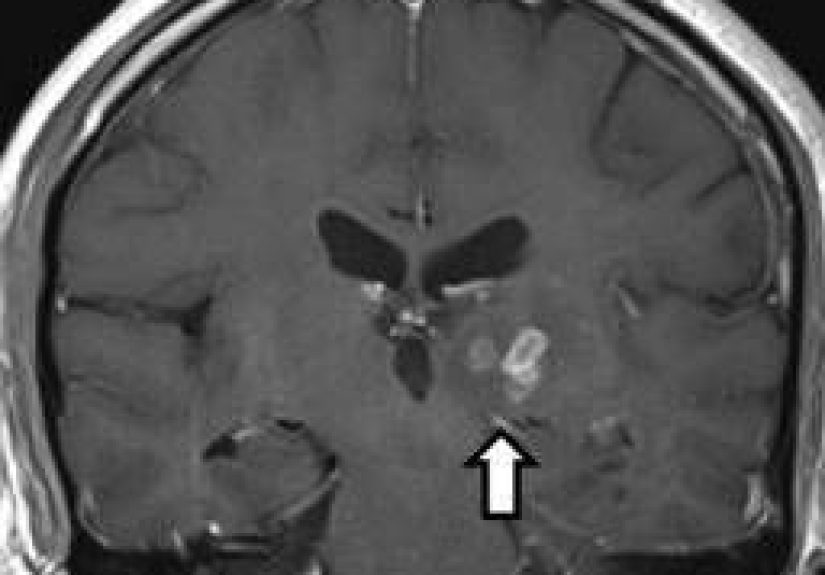
The patient was a 50-year-old man living in East England who experienced neurological symptoms, including headaches, seizures, memory problems, and progressive pain. Brain imaging showed abnormal lesions, but the cause was not obvious. Doctors considered several explanations, including inflammatory disease, cancer-like lesions, and more common parasitic infections such as neurocysticercosis.
The case became even stranger when scans suggested that the lesion had moved. Over roughly four years, the parasite appeared to travel about five centimeters from one side of the brain toward the other. That is not exactly a marathon by human standards, but inside the brain, five centimeters is a very dramatic commute.
Eventually, surgeons removed a small worm from the patient’s brain. The parasite was only about one centimeter long, but it carried a huge scientific surprise. Researchers at the Wellcome Sanger Institute and collaborating institutions used the tiny tissue sample to sequence the organism’s genome, creating the first genome sequence from this group of tapeworms.
What kind of tapeworm was found?
The worm was identified as Spirometra erinaceieuropaei, a species associated with sparganosis. Sparganosis is caused by the larval form of certain tapeworms, often called spargana. Unlike the adult tapeworms people usually imagine living in the intestine, spargana can migrate through tissues, causing inflammation and damage depending on where they travel.
Spirometra infections are rare in humans and are more commonly reported in parts of Asia. Known routes of infection include drinking contaminated water, eating raw or undercooked frogs or snakes, or using raw animal flesh as a traditional poultice. In the UK case, researchers could not prove exactly how the patient became infected, but his travel history made exposure in an endemic region plausible.
This parasite should not be confused with the pork tapeworm, Taenia solium, which is better known for causing cysticercosis and neurocysticercosis. Both can involve the brain, both can be serious, and both can make readers suddenly interested in handwashing. But they are different organisms with different life cycles, patterns of disease, and diagnostic challenges.
Why sequencing the tapeworm genome mattered
Genome sequencing is like reading an organism’s instruction manualexcept the manual is written in chemical letters, contains millions or billions of characters, and does not include a helpful index. In this case, the tapeworm’s genome was about 1.26 billion base pairs long, making it surprisingly large for a flatworm and much larger than scientists expected.
The genome gave researchers several important advantages. First, it confirmed the parasite’s identity with far more confidence than appearance alone. Second, it created a reference that could help diagnose future cases. Third, it gave scientists a way to inspect genes related to drug response, including possible resistance to some treatments and potential sensitivity to others.
That matters because rare parasites are difficult to treat when doctors do not know exactly what they are fighting. If the organism is unfamiliar, standard tests may come back negative. If the infection is in the brain, trial-and-error treatment becomes especially risky. The genome offered a more precise biological map.
What the DNA revealed about treatment
By analyzing the parasite’s genes, researchers looked for clues about how it might respond to existing anti-tapeworm drugs. The findings suggested that the worm may have natural resistance to benzimidazole drugs such as albendazole, a commonly used anti-parasitic medicine. At the same time, the genome suggested possible sensitivity to praziquantel, another drug used against tapeworms.
This does not mean every case can be solved by reading a parasite’s DNA and picking a pill like ordering from a menu. Brain infections are medically complex. Treatment may involve surgery, anti-parasitic drugs, corticosteroids to control inflammation, anti-seizure medications, and careful follow-up imaging. When parasites die inside sensitive tissues, the immune response itself can cause swelling and complications.
Still, the genomic information was a major step forward. It showed how sequencing can turn a rare medical oddity into useful scientific knowledge. One patient’s unusual diagnosis became a reference point for future doctors, microbiologists, parasitologists, and public health researchers.
Sparganosis vs. neurocysticercosis: what readers should know
Because “tapeworm in the brain” is a phrase that can cause instant panic, it is important to separate this rare sparganosis case from the more widely recognized condition neurocysticercosis.
Neurocysticercosis occurs when a person swallows eggs from Taenia solium, the pork tapeworm. The larvae can form cysts in the brain or central nervous system. Symptoms may include headaches, seizures, dizziness, confusion, nausea, vomiting, or other neurological problems. In many cases, symptoms appear months or years after infection, often when cysts begin to die and trigger inflammation.
A crucial point: eating undercooked pork can cause an intestinal pork tapeworm infection, but cysticercosis happens when someone swallows tapeworm eggs, usually through fecal contamination. That can occur through contaminated food, water, surfaces, or poor hand hygiene. This distinction is not just medical triviait affects prevention.
How doctors diagnose brain parasite infections
Diagnosis usually begins with symptoms and imaging. CT scans and MRI scans can show lesions, cysts, swelling, calcifications, or other signs of disease. Blood tests may help detect antibodies, although tests can vary in accuracy depending on the parasite, the stage of infection, and the number of lesions.
In rare cases like the Spirometra infection, standard tests may not identify the cause. That is where biopsy, surgery, microscopy, molecular testing, and genome sequencing can become essential. The UK case was especially difficult because the parasite was rare, unexpected, and not easily recognized by routine testing.
Doctors also look at travel history, food exposures, water sources, contact with infected individuals, and cultural or traditional practices that may increase risk. A patient’s medical story can be just as important as the scan on the screen.
Symptoms that should never be ignored
Most headaches are not caused by brain parasites. That sentence deserves a relaxing cup of tea. However, certain symptoms should always be taken seriously, especially when they are new, worsening, unexplained, or linked to travel or possible exposure.
Warning signs may include:
- New seizures or seizure-like episodes
- Persistent or worsening headaches
- Confusion, memory changes, or personality changes
- Unexplained weakness, poor coordination, or dizziness
- Vision problems, eye pain, or double vision
- Vomiting with severe headache
- Neurological symptoms after travel to regions where parasitic infections are more common
Anyone with these symptoms should seek medical care. Internet searches are useful for learning, but they are terrible at performing neurological exams. A qualified clinician can decide whether imaging, lab testing, specialist referral, or urgent treatment is needed.
Prevention: boring habits that actually work
The best parasite prevention advice is not glamorous, but it works. Wash your hands thoroughly after using the bathroom and before handling food. Wash fruits and vegetables. Drink safe water, especially when traveling. Avoid raw or undercooked meats, fish, reptiles, and amphibians. Cook meat to safe temperatures and use a food thermometer instead of the old “that looks fine” method, which has betrayed many home cooks throughout history.
Travelers should be especially careful in areas where sanitation is limited or where parasitic infections are more common. That does not mean being afraid of local food; it means being selective. Choose hot, freshly cooked meals. Be cautious with untreated water. Avoid unusual raw animal products. And if someone offers a raw frog poultice for your sore eye, perhaps politely choose modern medicine instead.
Why this case changed parasite research
The genome sequencing of Spirometra erinaceieuropaei showed how modern science can extract enormous value from a tiny sample. The worm itself was small, but its genome opened a new window into a poorly understood group of parasites.
For researchers, this matters because many neglected parasitic diseases receive less attention than they deserve. Rare infections can fall through diagnostic gaps. Doctors may never see a case during training. Laboratories may not have validated tests readily available. Patients may spend months or years searching for an explanation.
Genomic databases can help close that gap. When scientists sequence unusual organisms and share those data, future cases become easier to identify. A mysterious biopsy sample can be compared against known genetic references. Drug targets can be studied. Evolutionary relationships can be mapped. Public health surveillance can improve.
In other words, sequencing one worm can help the next patient avoid years of uncertainty. That is the kind of scientific progress that does not always arrive with fireworks, but it matters.
The human side of the headline
It is tempting to treat this story as a viral curiosity: “Brain worm! Click immediately!” But behind the headline was a real person with years of symptoms, frightening uncertainty, surgery, and recovery. Medical mystery stories are fascinating because they reveal how much science can do, but they also remind us how vulnerable patients can feel when symptoms do not fit a familiar pattern.
The best doctors are detectives, translators, and calm voices in chaotic moments. The best researchers take rare events and turn them into shared knowledge. The best public health messages keep people informed without making them want to live permanently inside a bubble.
This case sits at the intersection of all three: clinical care, genomic science, and prevention.
Experiences and practical reflections related to the brain tapeworm genome story
Stories like this tend to create two reactions. The first is horror, usually expressed as “Nope, absolutely not.” The second is curiosity: how did this happen, how did doctors find it, and what can ordinary people learn from it? The useful response is somewhere in the middle. We do not need panic, but we do need respect for rare infections, global travel, food safety, and the power of modern diagnostics.
One practical experience many travelers share is the “I’ll eat anything once” attitude. Adventurous eating can be a wonderful part of travel, but it should come with boundaries. Street food that is cooked hot in front of you is different from raw amphibian, untreated water, or mystery meat sitting at room temperature. The lesson is not to avoid culture; it is to avoid preventable risk. A memorable meal should become a good story, not a case report.
Another experience is the frustration of unexplained symptoms. People with recurring headaches, odd sensations, memory problems, or seizure-like events may first be told the issue is stress, migraine, fatigue, or anxiety. Sometimes that is true. Sometimes it is incomplete. The UK case shows why persistence matters when symptoms change, worsen, or do not respond to usual treatment. Patients should document symptoms, bring timelines to appointments, mention travel and food exposures, and ask what warning signs should trigger urgent care.
For clinicians, this case is a reminder that rare does not mean impossible. A doctor in a non-endemic country may not expect sparganosis, but travel, migration, and global food systems have made local assumptions less reliable. Asking about where a patient has lived, traveled, eaten, worked, and received traditional treatments can open diagnostic doors that imaging alone cannot unlock.
For families, the experience can be emotionally intense. Neurological symptoms are scary because they affect memory, movement, behavior, and independence. When the diagnosis involves a parasite, embarrassment may appear on top of fear. That stigma is unnecessary. Parasitic infections are biological events, not moral failures. Clear explanations and compassionate care help patients follow treatment and avoid shame.
For the public, the biggest takeaway is that simple habits remain powerful. Wash hands. Cook risky foods thoroughly. Use safe water. Take new seizures seriously. See a healthcare professional when neurological symptoms are unusual. And remember: the internet is excellent for learning the word “sparganosis,” but it is not a substitute for medical diagnosis.
Finally, the scientific experience is inspiring. A tiny worm removed from one patient became a genomic resource for the world. That is modern medicine at its best: turning an unsettling surprise into knowledge that may help someone else. The story may begin with a parasite in the brain, but it ends with better tools, smarter diagnosis, and a deeper understanding of life’s strange, sneaky, occasionally nightmare-fueling biology.
Conclusion
The world-first sequencing of a tapeworm removed from a man’s brain was more than a bizarre medical headline. It was a milestone in genomic medicine and parasite research. By decoding the DNA of Spirometra erinaceieuropaei, scientists confirmed the identity of a rare brain-invading parasite, studied possible drug responses, and created a valuable reference for future diagnosis and treatment.
The case also reminds us that rare infections require open-minded medicine, careful travel and food histories, and strong collaboration between surgeons, pathologists, genomic scientists, and infectious disease experts. For everyday readers, the practical advice is simple: practice good hygiene, choose safe food and water, cook animal products properly, and get medical care for serious neurological symptoms.
Yes, the phrase “tapeworm removed from man’s brain” may make your scalp tingle. But the real story is not fear. It is discovery. A frightening medical mystery became a scientific breakthroughproof that even the creepiest cases can push medicine forward.
Note: This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.






