Table of Contents >> Show >> Hide
- The Story Behind the Headline Is Bigger Than One Person
- What a Schizophrenia Diagnosis at 17 Can Really Mean
- Why Drawing Hallucinations Can Help
- What Real Treatment Usually Looks Like
- The Stigma Problem Is Still Huge
- Art Is Not a Cure, But It Can Be a Lifeline
- Additional Experiences Related to This Topic
- Conclusion
Generated with GPT-5.4 Thinking
Some headlines sound like they were written by a tabloid intern running on iced coffee and chaos. This one sounds like that at first glance. But underneath the dramatic wording is a very real, very human story about mental health, survival, and creative coping.
A schizophrenia diagnosis at 17 can feel like getting handed a life manual written in static. You are old enough to notice that something is wrong, young enough to feel blindsided by it, and probably already dealing with the regular circus of adolescence. School, identity, friendships, family pressure, hormones, future plans, and the general confusion of being a teenager do not exactly create a calm backdrop. Add psychosis into the mix, and daily life can start to feel unfamiliar, frightening, and exhausting.
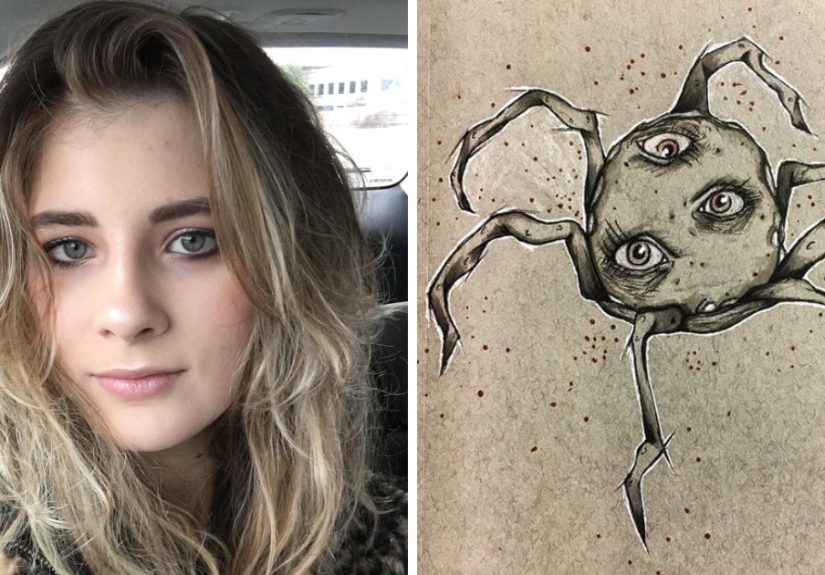
That is why stories about young people drawing their hallucinations hit such a nerve. They are not just about art. They are about translation. They are about taking something invisible, overwhelming, and hard to explain and giving it a shape on paper. A sketchbook becomes a witness. A drawing becomes evidence that the experience felt real, even when everyone around you insists it was not. For some people, that creative act does not erase the symptom, but it does lower the volume of the panic.
This article explores why that matters. It looks at what schizophrenia can actually mean in the late teen years, why drawing hallucinations may help some people cope, what treatment usually involves, and why public understanding still has a long way to go. The goal is not to sensationalize a diagnosis. It is to talk about it like grown-ups with Wi-Fi and compassion.
The Story Behind the Headline Is Bigger Than One Person
When a teenager says, “I started drawing my hallucinations to cope,” what they are really saying is, “I needed a way to make sense of an experience that words could not hold.” That idea matters because schizophrenia is still wildly misunderstood. Too often, public conversations flatten it into a horror movie stereotype, a punchline, or a scary plot device. Real life is far less cinematic and far more complicated.
For many people, schizophrenia is not one constant state of chaos. It can involve periods of distress, confusion, emotional blunting, withdrawal, sleep disruption, difficulty concentrating, and trouble separating what is real from what feels real. Symptoms may come and go, shift in intensity, or show up alongside anxiety, depression, or trauma-related stress. In other words, it is not a one-note condition, and the person living with it is never just their diagnosis.
That is part of what makes art such a compelling coping tool. A drawing can hold contradiction. It can be frightening and beautiful. Distorted and precise. Personal and still understandable to someone else. It says, “This is what my mind was doing,” without forcing the artist to reduce that experience to a tidy one-liner.
What a Schizophrenia Diagnosis at 17 Can Really Mean
Late adolescence is a common window for early symptoms
Schizophrenia often begins in the late teen years or early adulthood, which is one reason a diagnosis at 17 feels both shocking and medically plausible. This timing matters because it overlaps with major life transitions: finishing high school, planning college, starting work, learning independence, and trying to figure out who you are before the world asks for a five-year plan and a LinkedIn profile.
At that age, symptoms can be misread at first. Family members may think the teen is just moody, isolated, distracted, or rebellious. Teachers may see slipping grades. Friends may notice withdrawal or strange reactions but not know what to call them. Sometimes the person experiencing symptoms knows something feels off long before anyone else does. They may describe it vaguely as feeling disconnected, watched, confused, or like their brain is no longer behaving like it used to.
Symptoms are not personality flaws
One of the cruelest parts of schizophrenia stigma is how quickly symptoms get mistaken for character defects. Trouble organizing thoughts can be mistaken for laziness. Social withdrawal can look like rudeness. Flat emotion can be read as indifference. Fear can look like aggression. None of those assumptions help.
A teenager dealing with hallucinations is not being dramatic. A teenager struggling with paranoia is not automatically dangerous. A teenager who seems emotionally distant is not necessarily uncaring. These are symptoms, not moral failures. That distinction should be obvious, and yet society keeps failing the open-book test.
A diagnosis can be terrifying, but it can also be clarifying
Getting diagnosed with schizophrenia at 17 can feel like the floor dropping out. The word itself carries so much cultural baggage that some people hear the diagnosis and immediately imagine a ruined future. But for others, diagnosis also brings relief. It gives a name to a frightening experience. It opens the door to treatment. It can replace private confusion with practical next steps.
A label is not a destiny. It is a tool. And like every tool, it depends on how it is used. In the best cases, diagnosis becomes the beginning of support, not the end of hope.
Why Drawing Hallucinations Can Help
It turns fear into form
Hallucinations can feel intrusive because they arrive on their own terms. Drawing them flips that dynamic a little. The artist chooses the page, the line, the size, the color, the frame. That does not cure the symptom, but it can return a small sense of control. In mental health recovery, small control is not a small thing.
Think of it this way: when an experience is formless, it can feel endless. Once it is drawn, it becomes an object outside the body. A shape. A record. Something that can be observed rather than only endured. That shift can reduce distress for some people because it creates distance between the person and the symptom.
It helps communicate the hard-to-explain
Many people living with psychosis struggle to describe what they are going through. Language can feel slippery. Telling a parent, therapist, or doctor, “The room looked wrong,” may not fully capture the experience. A drawing, however, can communicate distortion, repetition, intensity, or emotional tone in a way ordinary conversation cannot.
That matters in treatment. Creative expression can help clinicians and loved ones better understand what the person is experiencing, how often symptoms occur, what triggers distress, and how those experiences affect daily life. Even when the drawing is abstract, it can still reveal patterns. Sometimes a scribble explains more than a speech.
It validates emotion without glamorizing illness
There is a huge difference between expressing suffering and romanticizing it. Drawing hallucinations can be validating because it says, “This was real to me.” It does not say, “This is glamorous.” Art can make room for fear, shame, confusion, grief, and anger without pretending any of those feelings are cute or poetic in a Pinterest-board way.
That is one reason creative coping deserves respect. It acknowledges the experience honestly while still moving toward safety and self-understanding. It is not denial. It is not surrender. It is a way of saying, “I am still here, and I am trying to work with what my mind is doing.”
What Real Treatment Usually Looks Like
Art can help, but it is usually not the whole plan
Drawing can be powerful, but it is not a replacement for treatment. Schizophrenia is typically managed with a combination of medical care, therapy, education, routine, and support. For many people, antipsychotic medication plays a central role in reducing the intensity or frequency of psychotic symptoms. Therapy can help with insight, stress management, coping strategies, and everyday functioning.
This is where a lot of online conversations go sideways. People love a dramatic coping story because it is visually striking and emotionally shareable. But the most helpful truth is less flashy: recovery often depends on consistent, boring, deeply unglamorous support. Medication reviews. Therapy appointments. Sleep. School accommodations. Family education. Follow-up care. Stability. Not exactly viral content, but life-changing all the same.
Early intervention matters
When psychosis shows up for the first time in adolescence or young adulthood, early treatment can make a major difference. Coordinated specialty care programs for first-episode psychosis are designed to support people early, often with a team-based approach that includes therapy, medication support, family education, and help with school or work. The point is not simply to reduce symptoms. It is to protect the person’s future while they are still building it.
That is especially important at 17, when interruption can feel enormous. Missing school, losing social confidence, withdrawing from everyday life, or feeling misunderstood can all add secondary damage on top of the symptoms themselves. Good care tries to prevent that pileup.
Family and environment matter more than people think
A supportive environment does not magically fix schizophrenia, but it can absolutely change the recovery experience. Teens do better when the adults around them learn what symptoms look like, reduce blame, encourage treatment, and avoid treating the diagnosis like a family scandal that must be hidden behind the curtains with the fancy dishes.
Structure helps too. Regular sleep, reduced substance use, manageable stress, and predictable routines can make coping easier. So can having safe ways to express distress. For one person that may be drawing. For another it may be music, journaling, movement, or peer support. Recovery is not one-size-fits-all, and thank goodness for that, because human beings have never once behaved like matching storage bins.
The Stigma Problem Is Still Huge
One reason stories like this resonate is that they push back against stereotypes. Popular culture has done a spectacularly bad job portraying schizophrenia. Too many depictions confuse it with other conditions, exaggerate violence, or reduce the person to a set of frightening symptoms. That kind of framing does real damage. It makes people less likely to seek help, more likely to hide symptoms, and more likely to internalize shame.
A teen artist drawing hallucinations for coping offers a different image: a person with insight, creativity, fear, intelligence, and agency. That matters. It reminds the public that schizophrenia does not erase personality, talent, humor, or ambition. Someone can live with psychosis and still make art, go to school, build relationships, and contribute meaningfully to the world.
Representation alone is not treatment, but it can change the climate around treatment. And sometimes that climate is the difference between silence and support.
Art Is Not a Cure, But It Can Be a Lifeline
Research on formal art therapy for psychosis is still developing. The evidence is mixed, and experts do not present it as a magic fix. But that does not make creative coping trivial. In real life, many people describe art as a practical way to regulate emotion, externalize fear, and communicate experiences that feel too strange or too personal to explain directly.
That is why the image of a 17-year-old drawing hallucinations is so powerful. It captures a simple truth: when the mind becomes difficult to trust, creating something tangible can help rebuild a sense of self. The page says, “You are more than what is happening to you.” The act of making says, “You still have choices.”
And that may be the most important point of all. Schizophrenia can disrupt reality, but coping strategies like drawing can restore a little authorship. Not total control. Not instant recovery. Just authorship. Sometimes that is where healing begins.
Additional Experiences Related to This Topic
People who are diagnosed with schizophrenia in their teens often describe the period before diagnosis as confusing rather than dramatic. It may start with subtle changes: sleep gets worse, concentration slips, ordinary sounds feel unusually loaded, or social situations become exhausting. A student who used to be organized may begin missing assignments. A friend who used to joke constantly may go quiet. Family members sometimes interpret these changes as stress, burnout, attitude, or typical teenage behavior. The person experiencing them often senses that something deeper is wrong but cannot explain it clearly. That gap between internal distress and outside perception can be incredibly isolating.
After diagnosis, many young people report having two parallel battles. The first is the condition itself: managing hallucinations, intrusive thoughts, fear, emotional numbness, or disorganized thinking. The second is everyone else’s reaction. Some people feel relieved to finally have a diagnosis. Others feel crushed by the stereotypes attached to the word schizophrenia. They worry they will be seen as dangerous, unstable, or incapable. They may start editing themselves in conversations, hiding symptoms from friends, or avoiding treatment because they do not want to be reduced to a label. In that sense, stigma becomes its own symptom multiplier.
Creative expression often enters during this stage because it offers something that ordinary conversation does not. A drawing, collage, painting, or visual journal can capture distortion, repetition, fear, fragmentation, or sensory overload without forcing the person to narrate every detail out loud. Many people say that when they create an image of what they experienced, the experience feels less chaotic. It becomes something they can look at from a distance. Some keep that work private. Others share it with therapists, family members, or online communities to help others understand what living with psychosis can feel like on the inside.
Another common experience is grief. Teenagers diagnosed with schizophrenia may grieve the version of life they expected to have. They may worry about school, dating, independence, work, or whether they will ever feel “normal” again. That grief is real, and it deserves space. At the same time, many people eventually describe building a new definition of normal that includes treatment, creative coping, supportive relationships, and a better understanding of their own warning signs. Recovery is rarely a clean upward line. It tends to look more like progress, setbacks, adjustments, and learning what helps.
What stands out in many real-world accounts is not perfection but persistence. People find routines that steady them. They learn which stressors make symptoms worse. They discover that peer support can reduce shame. They work with clinicians who take their experiences seriously. They create art not because suffering is beautiful, but because turning pain into form can make it survivable. That is the deeper meaning behind stories like this one. The drawing is not the whole recovery. It is evidence that the person is still reaching for connection, clarity, and control.
Conclusion
“I was diagnosed with schizophrenia at 17, so I started drawing my hallucinations to cope with it” is a headline that grabs attention, but its lasting value is not shock. It is honesty. It opens a window into what psychosis can feel like, what adolescence can magnify, and how creativity can become a practical survival tool. Drawing does not replace treatment, and it should not have to. But as part of a broader care plan, it can help transform fear into expression and confusion into communication.
The larger lesson is simple: people living with schizophrenia are not stereotypes, plot twists, or cautionary tales. They are people. Some of them are artists. Some are students. Some are quietly trying to make it through the week while learning how to trust their own minds again. The more accurately we talk about schizophrenia, the easier it becomes for people to seek help early, stay connected, and build lives that are not defined only by symptoms.
![18 Best Types of Charts and Graphs for Data Visualization [+ How to Choose]](https://corkopencoffee.org/wp-content/uploads/2026/05/18-best-types-of-charts-and-graphs-for-data-visualization-how-to-choose-qKM1PBYG-thumb.jpg)




